A study in JAMA Psychiatry explores how functional MRI (fMRI) biomarkers can help distinguish major depressive disorder (MDD) 😔 from healthy individuals. Researchers found that regional homogeneity (ReHo) patterns in the brain are a more reliable marker for MDD than traditional structural MRI 🏗️.
🔬 Why does this matter? 👉 Better Diagnostics: fMRI could lead to more objective ways to diagnose depression, reducing reliance on self-reporting. 👉 Early Detection: One day, brain scans 🏥 might help identify people at risk before symptoms fully develop. 👉 Personalized Treatment: Understanding individual brain patterns could help guide targeted interventions like therapy or medication.
Could brain scans be the future of depression diagnosis? 🤔 Drop your thoughts below! ⬇️
A recent 8-week double-blind, randomized, placebo-controlled trial investigated whether oral creatine monohydrate (5g/day) could enhance the effects of cognitive-behavioral therapy (CBT) in treating major depressive disorder (MDD)—especially in under-resourced areas where access to treatment is limited.
🔬 Why Does This Matter? While CBT is a gold-standard therapy for depression, many patients do not achieve full remission. This study explored whether creatine—widely used for muscle and brain energy metabolism—could provide an extra boost to treatment.
🧠 Key Findings: ✅ Participants receiving creatine + CBT had greater reductions in depression symptoms (measured by the Hamilton Depression Rating Scale) compared to those receiving placebo + CBT ✅ Reported improvements in mood, energy levels, and cognitive function ✅ Creatine was well-tolerated, with no significant safety concerns ✅ CBT was delivered once weekly by trained therapists
⚠️ Study Limitations: 🔹 Small sample size—larger studies are needed to confirm these findings 🔹 Short trial duration—long-term effects are still unknown 🔹 Study population—results may not generalize to all individuals with MDD
💡 What’s Next? If larger studies confirm these results, creatine could become an accessible, affordable adjunct to therapy, particularly in communities with limited mental health resources.
What do you think? Could a common fitness supplement help improve mental health? Let’s discuss! ⬇️
Gepirone may have flown under the radar for many of us. I’ll admit, it didn’t generate much excitement on my end. However, it recently crossed a significant milestone: FDA approval as an antidepressant. But let’s not overlook its rocky path to getting there—a journey marked by hurdles and setbacks.
The road to FDA approval for gepirone was anything but smooth. Its initial development began decades ago, but the approval process faced repeated delays and rejections. Questions about efficacy and study designs kept it in limbo for years. What ultimately got it across the finish line was a re-analysis of data demonstrating robust effects in specific populations, particularly those with significant depressive symptoms. This serves as a reminder that persistence and rigorous data reassessment can change the trajectory for medications once thought to have limited potential.
Now that gepirone is finally available, the big question is: should we care? If so, where does it fit into our treatment algorithms for adult depression?
With a mechanism targeting the serotonin 1A receptor as a partial agonist, gepirone offers a unique profile compared to SSRIs, SNRIs, and other standard antidepressants. Its anxiolytic effects may make it particularly appealing for patients with co-occurring anxiety. However, like any medication, it isn’t without its downsides.
Potential side effects include nausea, dizziness, fatigue, and headache. These are generally mild, but it’s important to monitor for tolerability in sensitive patients. Gepirone also carries warnings about potential interactions with other serotonergic agents, raising the risk of serotonin syndrome. While this risk isn’t unique to gepirone, it’s a critical point to keep in mind when integrating it into a treatment plan.
So, where does gepirone fit? Will it serve as a first-line option for certain patients, or will it find a niche role for those with specific tolerability issues or suboptimal responses to other antidepressants?
I’d love to hear your thoughts. Is gepirone a tool worth adding to our arsenal, or just another option that might not shift the needle much in clinical practice?
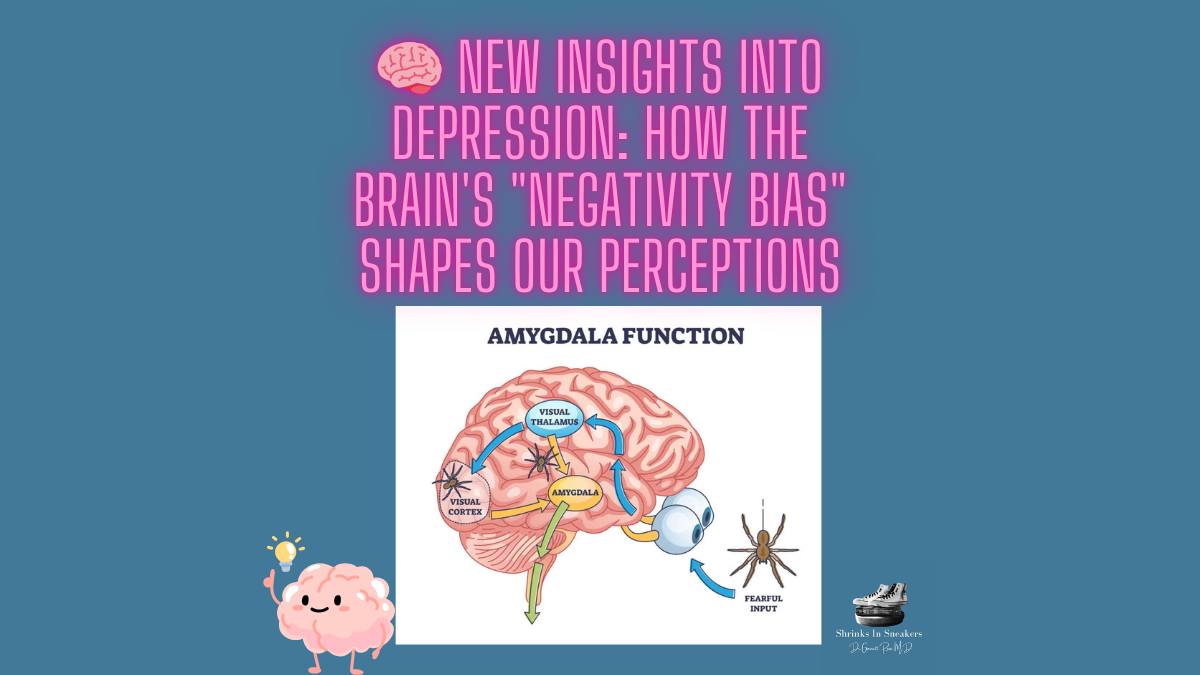
Did you know that in depression, the brain’s wiring can actually amplify negative experiences? Recent research from the Institut Pasteur and collaborators explored this phenomenon, finding that depression alters specific neurons in the amygdala. These changes can reduce activity in neurons that process positive stimuli while overactivating those that process negative stimuli. This “negativity bias” means people with depression often perceive even neutral events through a negative lens.
In studies with mouse models of depression, activating neurons responsible for positive perceptions helped reduce depressive behaviors. This groundbreaking discovery could pave the way for new treatments aimed at rebalancing these circuits, especially for people who don’t respond to conventional therapies.
By understanding depression’s effects on the amygdala, researchers hope to develop more targeted and effective therapies for those resistant to current treatments. This is a step toward a more personalized approach to mental health.
Stage 1: more than one adequate trial of 1 major class of antidepressants
Stage 2: Failure of more than 2 adequate trials of two different classes of antidepressants
Stage 3: stage 2 + TCA
Stage 4: Stage 3 + MAOI
Stage 5: Stage 4 + bilateral ECT
With every medication or neuromodulation procedure used that doesn’t work, the more treatment resistant the depression becomes.
Antidepressant Response Rates
Frist Medication Trial: 50% respond and 37% have remission
Second Medication Trial: Another 29% respond and 31% have remission
Third Medication Trial: 17% respond and 14% have remission
Fourth Medication Trial: 16% respond and 13% have remission
The overall cumulative remission rates are 67%, keeping in mind that people who progressed through more treatment stages had higher relapse rates and more residual symptoms including anhedonia, emotional blunting, and lack of motivation.
If someone is having a poor response to medication, what do you do?
We know that bipolar disorder is missed in a significant number of patients who present with depression about one in five will be misdiagnosed. We also know that antidepressants can be mood destabilizing in bipolar illness resulting in mixed features and rapid cycling. Other things that can interfere with response include substance use disorder, personality traits, and PTSD.
Medical Comorbidities that can interfere with antidepressant response include hypothyroidism, Cushing disease, Parkinson’s disease, cancer, vitamin/nutritional deficiencies, and viral infections
Psychosocial factors that contribute to treatment resistance
-Female sex
-Older Age
-Single Unmarried (happiness studies indicate that good relationships are very important)
-Unemployment
Symptoms that make TRD more Likely
-Recurrent episodes usually 3 or more
-Severe depression and inpatient admission
-Anxiety, Insomnia, or Migraine
When Your First Choice Fails
There are several approaches
-Switch antidepressant classes
-Combine antidepressants
-Add a dopamine blocking medication
-Add L-methylfolate
-Add Psychotherapy
-Start Neuromodulation
What’s the most effective strategy
Hands down the most effective thing to do if a patient has a poor response to the initial antidepressant treatment is to add a dopamine blocking medication. Response and remission rates are much higher, but it comes at the price of increased side effect potential.
What are the most used Dopamine Blockers in Antidepressant Augmentation
-Quetiapine
-Olanzapine
-Risperidone
-Aripiprazole
-Ziprasidone
Older patients 65 years and older respond better to aripiprazole augmentation than switch to bupropion, or combination with bupropion.
Brexpiprazole: 1-3 mg/day Adjunctive for Depression
Most Common Concerns patients have about being on dopamine Blocking Medication
-Weight gain 60% of people report this concern
-Metabolic side effects
-EPS
-Sedation
-Akathisia
-Prolactin-related Effects
Anti-Inflammatory Medications
For those with elevated inflammatory biomarkers specifically c-reactive protein there is some emerging evidence that these treatments work.
-Medications like Celecoxib, Omega-3 fatty acids, statin drugs and minocycline
-Weight loss
-Effect Size: 0.55
-Higher response and remission rates
-May only work in those with high inflammatory biomarkers
Glutamate Modulators
-Ketamine Infusions and Esketamine: both work and a reasonable option if TRD
-There are several medications in development
Psychotherapy in TRD
Unfortunately, what we find with TRD is psychotherapy does not prevent TRD, it doesn’t mean there is no benefit it just means future episodes will not be prevented by psychotherapy. On its own, psychotherapy may not be as helpful as we would like in TRD but when combined with medication it does help. That tells us about the importance of evaluating severity of depressive episode.
When Someone does not experience remission from major depression, we need to ask ourselves why, and come up with new solutions. This discussion will focus on the treatment of these individuals by first explaining what symptoms predict poor response to treatment and what symptoms of major depression result in the most psychosocial dysfunction.
What Causes Functional Impairment in Major Depression
From the STAR*D study we know that only 50% of patients respond to the first antidepressant treatment and only 33% achieve remission. An important question is why, or more specifically what factors result in poor outcomes.
Contrary to popular belief the medications we use to treat depression work well for some neurovegetative symptoms. Symptoms such as sleep, and appetite improve but the most debilitating symptoms often remain. Consistently Anhedonia and concentration are rated by patients with depression as the most debilitating. These cognitive symptoms such as trouble concentrating, difficulty planning, and poor attention lead to dysfunction at home and work.
Cognitive Symptoms Impair Work Performance
We all need to work to live, and depression is a leading cause of disability and poor work performance worldwide. What we know is that subjective measures of cognitive dysfunction are a better predictor of workplace performance than total depression severity. Someone with more severe overall depression scores may perform better at work than someone with perceived cognitive dysfunction from depression. This is one possible reason for a lack of improvement as many treatments do not address cognitive symptoms.
Anhedonia makes everything Worse
Possibly the most debilitating symptom of depression is anhedonia. Anhedonia is defined as loss of interest in previously pleasurable activities. A strong predictor of poor antidepressant outcome is the loss of interest. Making anhedonia a primary target of treatment would be wise if we want to improve outcomes in depression.
We have additional evidence that indicates how important anhedonia is for psychosocial function. Functional improvement is strongly associated with improvement in anhedonia. The improvement in anhedonia had a larger effect on psychosocial function than overall symptomatic response.
Emotional Blunting Effects on Treatment Outcomes
While people do not want to be depressed, they also do not want to be emotionally dull. Unfortunately, we know that emotional blunting is reported in nearly half of all depressed patients on antidepressants. This appears to be common to all monoamine antidepressants with bupropion having the lowest reported risk. Emotional blunting cannot be totally accounted for as just a side effect of treatment, it’s also a symptom of depression. However, the point remains the same emotional blunting results in poorer quality of remission.
Doctors Are Too Medically Oriented
The world of psychiatry is very different from other medical specialties. Psychiatry is really art based in science and if you try to approach mental health treatment from a strictly scientific basis you will never help anyone. When patients and physicians are asked to rank the symptoms of depression, they believe are most important, the lists do not match up.
Patients focus on restoration of positive affect by ranking things such as meaning and purpose in life, enjoyment in life, satisfaction with oneself as the top three most important things to address in depression. Clearly what should stand out to you here is that medication is unlikely to improve any of these factors.
Doctors rank depressed mood, hopelessness, and anhedonia as their top three symptoms to address. These symptoms are far better addressed by medication than the ones listed by patients although you could argue that hopelessness and anhedonia are difficult to treat with medication.
The effect of Loneliness on Health Outcomes
I’ve talked about this before and it continues to be a major concern in our modern world. We are the most connected we have ever been as a society with the advent of social media and the internet, yet no one feels connected. This is an existential crisis for all of us and I haven’t heard many good solutions. Time and time again we go back to the same things such as the internet and social media to feel connected and they continue to let us down. Not only is this emotionally taxing, but it’s also effecting our physical health as well. Here is yet another example of something that is very important for depression treatment outcomes that medication cannot fix.
Conclusion
What does this all mean? Should we stop attempting to use medication for the symptoms of depression? For me these findings indicate we need to screen more carefully for these specific symptoms that result in poor outcomes. We need to improve our psychosocial treatments to help people address ways to enhancing meaning and purpose in their lives. We need to recognize the limitations of medications. Medications have a place and do address some of the symptoms associated with depression, they just aren’t the ones patients believe are most important in their lives.
Major Depressive Disorder (MDD) With Psychotic Features
This is a diagnosis that I often receive questions about. It can be confusing, how do we know if the person has schizophrenia, schizoaffective disorder, or bipolar disorder with psychotic features?
They all have psychotic symptoms such as delusions and hallucinations.
In this video I’m going to explain how we navigate this diagnostic dilemma.
For one to be diagnosed with MDD with psychotic features they must meet criteria for major depressive disorder based on the DSM-5TR.
As a reminder, to meet criteria the person must have 5 out of 9 symptoms within a two-week period and at least one symptom must be either depressed mood or loss of interest.
In medical school they teach you the mnemonic SIGECAPS, an interesting fact is this is written the way you would fill out a paper prescription for depression. SIG Energy Capsules which you would give to a person with major depression because of the low energy and loss of interest commonly seen in major depression.
Anyway…
The other criteria include
-Weight loss or weight gain
-Insomnia or hypersomnia
-Psychomotor agitation or retardation
-Fatigue or loss of energy
-Feelings of worthlessness or guilt
-Poor concentration
-Recurrent thoughts of death or suicidal ideation
So, we have a person who meets criteria for MDD, they have 5 out of 9 symptoms for a two-week period.
We should keep in mind it’s important that the person has also suffered some loss of function in their personal or professional life because of the symptoms. This is what makes it a disorder.
Now, what if the person also has a loss of reality-based thinking in conjunction with the major depressive episode?
This will include things like delusions and hallucinations. The delusions can be persecutory in nature or paranoid, but other types may occur too. The persecutory delusions are ones where the person feels attacked or victimized by others. They may even believe people are coming into their home to harm them. This usually presents with the patient reporting things being moved in the home or things being out of place. A common paranoid delusion is one where the person believes they are being followed. This usually presents as a car or person the patient keeps seeing, and they cannot believe that it may just be a coincidence, or someone who travels the same route to work every day.
Delusions are fixed false beliefs, and although there may be rational explanations for the things going on around them, this is the patient’s reality, and you must be careful when challenging it. The belief is fixed, and That is why presenting evidence contrary to the belief is not effective.
The important point here is the psychotic symptoms are only present during the major depressive episode. Treat the depression and the psychotic symptoms resolve. If the psychotic symptoms remain after the major depressive episode is successfully treated, you need to reevaluate the diagnosis.
This is what separates MDD with psychotic features from schizophrenia.
In bipolar disorder with psychotic features, the psychosis often occurs in the manic phase of the illness and has a grandiose theme associated with it. The patient my for example believe they are a prominent religious figure, or the government is plotting against them.
We often call the delusions in depressive episodes mood congruent, meaning they are consistent with how the person is feeling. It’s not a far stretch for a person who is severally depressed to feel like people want to harm them.
Treatment
Treatment is well established and consists of an SSRI or other antidepressant medication in combination with a dopamine blocking medication. The other option is electroconvulsive therapy (ECT) when the person is severally depressed not eating, attending to ADLs, or at risk for suicide.
Patients should remain on medication for at least 6 months after complete resolution of symptoms. This is very important as relapse has been proven to occur when medication is stopped prior to that time. People can taper off the dopamine blocking medication after 6 months as these tend to have worse side effect profiles. The SSRI should be continued for 1 year at which time you can attempt to taper off or reach a lowest effective dose if symptoms begin to reappear. An index phase of ECT should be completed if that is the treatment of choice which consists of 12 total sessions done either 2 or 3 times per week.
This is the beginning of a series on depressive disorders starting with MDD. I want to keep the posts short and to the point, less than 500 words each.
Major depressive disorder (MDD) is very common. The lifetime and 12-month prevalence are 13-17% and 6-7% in American adults over the age of 18. For adults under the age of 50, it’s twice as likely to affect females when compared to males. MDD is associated with high rates of psychiatric and medical morbidity, impaired work function, and disability.
DSM-5 Criteria for Diagnosis
To diagnose MDD you must have at least 5 of the following symptoms over the same two-week period. At least one of the symptoms must be depressed mood or loss of interest.
The symptoms are as follows, depressed mood; diminished interest in pleasurable activities; changes in appetite either increased or decreased; insomnia or hypersomnia (increased sleep); psychomotor agitation (restlessness) or retardation (slow movement); decreased energy; guilt or feelings of worthlessness; diminished ability to concentrate; and recurrent thoughts of suicide. These symptoms must occur every day or nearly every day and last all day over that same two-week period. The symptoms can be either a subjective account, observed by others, or some combination of both.
It must cause significant disruption in social, occupational, and other important areas of function. It cannot be caused by a medical condition or substance use.
Specifiers for MDD:
Mild; Moderate; Severe; without psychotic features; Severe with psychotic features; in partial remission; in full remission; chronic; with catatonic features; with melancholic features; with atypical features; with post-partum onset; with or without full inter-episode recovery; and with seasonal pattern.
In the next post we will cover the highlighted specifiers and what specific symptoms separate them from each other. Please like, share, and comment we want to hear from you.