Evidence Supporting Overprescription
- Prescribing Without Meeting Diagnostic Criteria
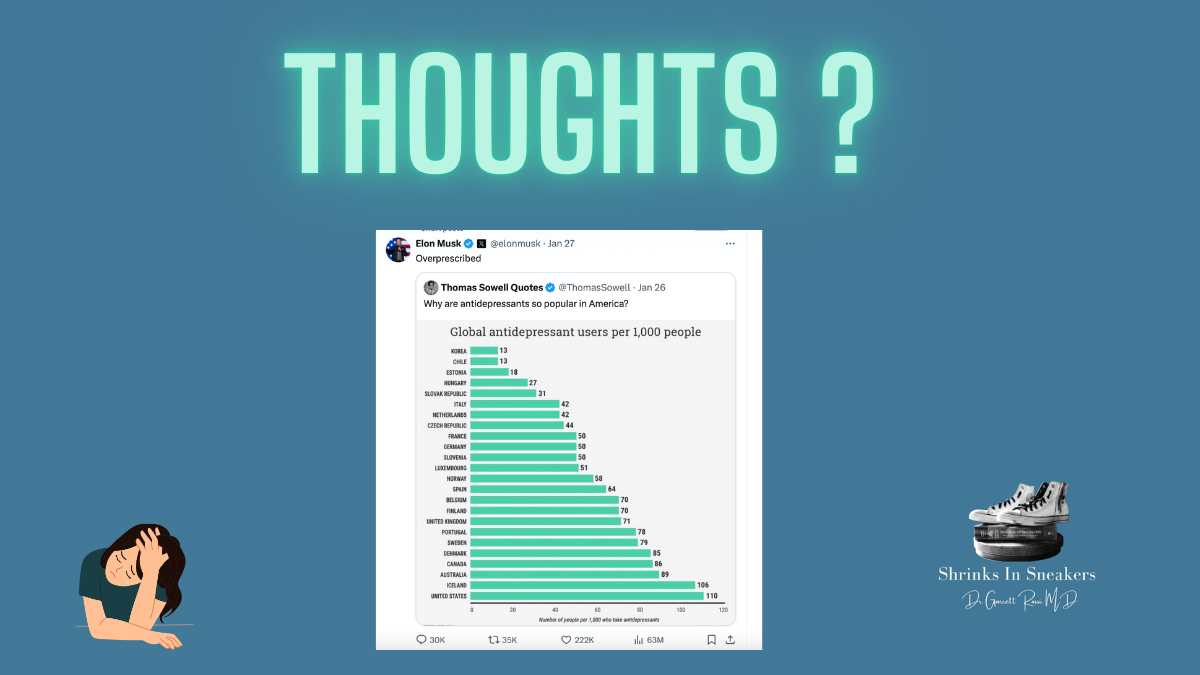
- A 2011 study published in Health Affairs found that only 38.4% of patients prescribed antidepressants met criteria for major depressive disorder (MDD), based on the National Ambulatory Medical Care Survey. Many prescriptions were given for milder depressive symptoms or anxiety disorders, suggesting potential overprescription.
- Subclinical Depression: Some prescriptions were issued for symptoms that did not meet the diagnostic threshold for any psychiatric disorder.
- Primary Care Prescribing Patterns
- Antidepressants are frequently prescribed in primary care settings, where diagnostic accuracy may be lower than in psychiatric settings.
- A 2020 review in JAMA Internal Medicine highlighted that primary care physicians write 79% of antidepressant prescriptions in the U.S., and these are often issued without consultation with a mental health professional.
- Off-Label Use
- A 2016 study in JAMA Psychiatry found that 30% of antidepressant prescriptions are for off-label indications like insomnia, chronic pain, or fatigue, despite limited evidence supporting their efficacy for many of these uses.
- Prolonged Use
- Many individuals take antidepressants for extended periods without regular reassessment. A 2019 study in The British Journal of Psychiatry noted that long-term antidepressant use often continues without clear ongoing benefit, raising questions about whether prescriptions are monitored effectively.
Evidence Suggesting Appropriate or Underprescription
- Untreated Mental Illness
- The World Health Organization (WHO) estimates that nearly 50% of individuals with depression in high-income countries, including the U.S., do not receive treatment.
- A 2017 study in JAMA Psychiatry found that many individuals with severe depressive symptoms go untreated, particularly in low-income or minority populations.
- Misperceptions of Overprescription
- A 2020 meta-analysis in The Lancet Psychiatry showed that antidepressants are highly effective for moderate-to-severe depression, and their increased use could reflect improved treatment of these conditions rather than overprescription.
- Increased public awareness of mental health has led to more people seeking care, which may explain higher prescription rates.
- Use in Non-Psychiatric Disorders
- Antidepressants, particularly SSRIs and SNRIs, are evidence-based treatments for anxiety disorders, PTSD, OCD, and some chronic pain conditions. Their prescription for these conditions might be misinterpreted as “overprescription.”
Balancing Perspectives
The evidence suggests a mixed picture:
- On one hand, antidepressants are sometimes prescribed without meeting diagnostic criteria or for off-label uses with weak supporting evidence.
- On the other hand, a significant proportion of individuals with moderate-to-severe depression or anxiety remain untreated, indicating possible under prescription in certain populations.
Scientific Consensus
The issue may stem less from overprescription overall and more from suboptimal prescribing practices, including:
- Prescribing antidepressants where psychotherapy or other treatments might be more appropriate.
- Inadequate follow-up or reassessment of long-term users.
- Limited mental health training for primary care providers, who are often the frontline prescribers.