The question of whether antidepressants are overprescribed in the United States is complex and depends on how “overprescription” is defined.
Arguments Suggesting Overprescription
- Broad Diagnostic Criteria:
- The criteria for diagnosing conditions like major depressive disorder (MDD) can be broad, potentially leading to overdiagnosis and, consequently, overprescription.
- Prescribing Practices:
- Primary care physicians write most antidepressant prescriptions, often without thorough psychiatric evaluation.
- Some prescriptions are written for mild cases of depression or subclinical symptoms where psychotherapy or lifestyle changes might suffice.
- Off-Label Use:
- Antidepressants are frequently prescribed off-label for conditions like insomnia, chronic pain, or anxiety, contributing to their high utilization.
- Pharmaceutical Influence:
- Aggressive marketing by pharmaceutical companies has historically played a role in increasing antidepressant use.
Arguments Against Overprescription
- Underdiagnosis and Undertreatment:
- Despite high prescription rates, many individuals with diagnosable depression or anxiety disorders go untreated, particularly in underserved populations.
- Stigma and access barriers often prevent people from seeking care.
- Increasing Mental Health Awareness:
- Growing awareness of mental health issues may explain rising prescription rates, as more people seek help for legitimate conditions.
- Non-Psychiatric Indications:
- Antidepressants are also effective for non-depressive disorders, like obsessive-compulsive disorder (OCD), post-traumatic stress disorder (PTSD), and chronic pain, which justifies some of their broader use.
Data on Antidepressant Use
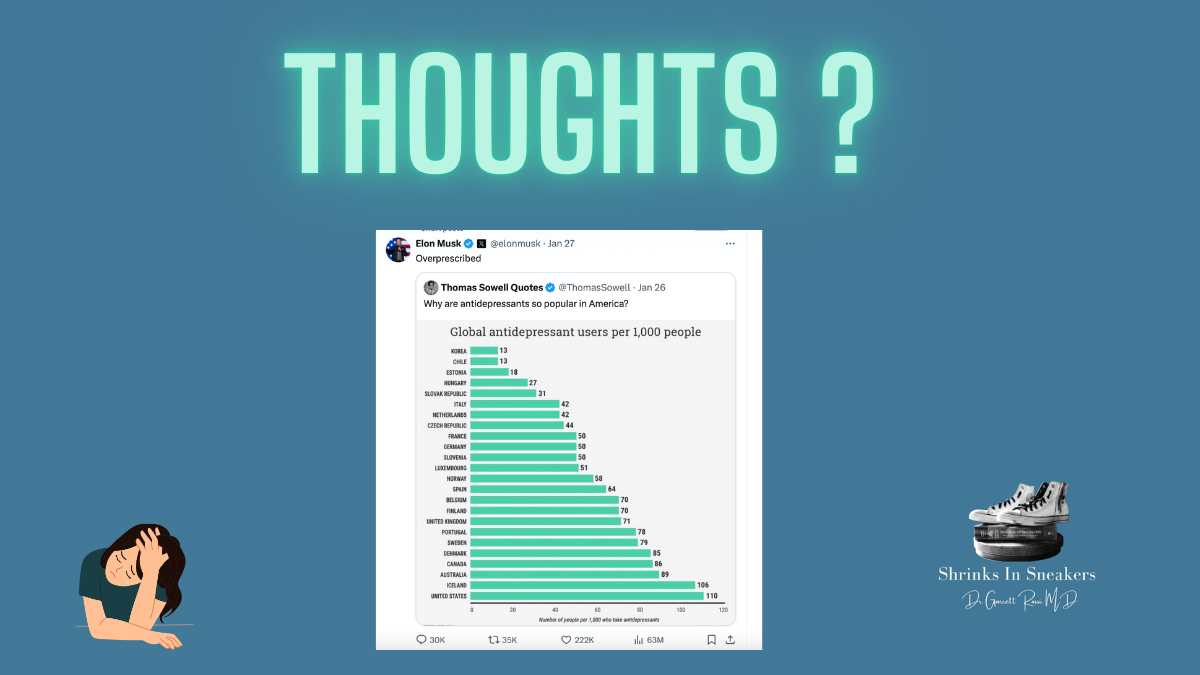
According to surveys, about 1 in 8 Americans aged 18 and older take antidepressants, and usage is particularly high among women, especially those aged 40–59. While this might seem like a high prevalence, it may also reflect greater recognition and treatment of mental health issues.
Key Considerations
- Patient-Centered Care: The decision to prescribe antidepressants should be tailored to the individual, based on a comprehensive assessment of their symptoms and needs.
- Access to Alternatives: Many individuals lack access to evidence-based non-pharmacological treatments like psychotherapy due to cost, availability, or stigma, making antidepressants a more feasible option.
- Role of Education: Educating both prescribers and patients on appropriate use can reduce potential overprescription.